




What is Heart Valve Surgery
Criteria Considered in Heart Valve Selection and Valve Types
The introduction of prosthetic heart valves has been a great development for heart valve patients and it has been possible to restore the health of many patients who could not find a treatment chance with surgery. Currently, efforts to make the ideal prosthetic heart valve continue very intensely, and at the end of tissue and genetic engineering studies, the vision of producing a valve from the cells of patients when necessary is close to becoming a reality. Today, we can divide prosthetic heart valves into two groups: Mechanical and Bioprosthetic heart valves.
What should an ideal prosthetic heart valve be like?
When the valve is installed, it should be durable and functional for a long time, should not cause clot formation in the body, should be easy to install during surgery, should not cause leakage from the valve edges, should not cause hemolysis and be resistant to infection.
The choice of the valve to be fitted depends on the patient’s preference, age of the patient, characteristics of the prosthetic valve, availability, cost and the surgeon’s preference.
In general, functional impairment is observed in heart valves due to stenosis and / or failure.
While aortic stenosis (stenosis) is the most common aortic valve disease, the most common mitral valve disease is mitral insufficiency.
Valve surgery options
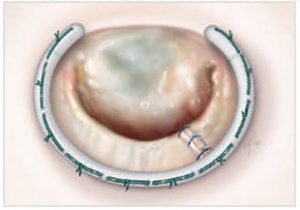
Generally, two options are emphasized: valve repair or replacement with a prosthetic valve.
If it was up to us, we would prefer to repair all valves and allow the patients to maintain their own tissues without being exposed to foreign matter.
Unfortunately, we can rarely repair aortic valves, whereas mitral valves can be repaired more often.
Prosthetic valve selection
Generally, two options are available: mechanical (metal) valves and bioprosthesis (tissue) valves.
Well, which types of metal and tissue prosthetic heart valves should you choose?

Mechanical (metal) heart valves
– Advantages
They can be manufactured in various sizes and are easily obtained.
Metal covers are generally easy to fit.
Mechanical valves are rarely distorted and usually do not need to be replaced with a second operation.
They do not require special anti-reaction drugs, as they are not recognized as foreign substances by the body.
– Disadvantages
The main disadvantage is that they are thrombogenic, a patient with a mechanical heart valve must use Coumadin (anti-coagulant) every day, otherwise, a clot can occur in the inserted valve and generate bad results. When using Coumadin, you should also be careful with your food and the medicines you use, as some foods and medications can decrease or increase the anti-coagulant effect of Coumadin. Blood tests should be performed for PT-INR values at regular intervals to evaluate the effectiveness of Coumadin treatment and to make dose adjustments.
In addition, coumadin is a teratonegic drug, it is not prescribed for pregnant women, they are not very suitable valves for young female patients of childbearing age.
Finally, mechanical valves often generate a special mechanical prosthetic heart valve sound that can be heard by the patient himself or by those around him. Patients sometimes complain about this noise.
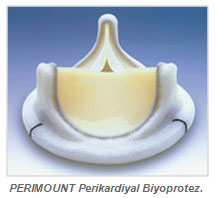
Bioprosthesis (tissue) heart valves
– Advantages
A patient who has been fitted with a tissue cover does not need to use anti-coagulants (Coumadin) after the procedure, although some surgeons do subject their patients to Coumadin therapy for 8-12 weeks after surgery until the tissues have fully healed.
In the long run, daily Aspirin is enough. This way, the risk and follow-up discomfort of long-term use of anti-coagulant drugs are eliminated.
The fact that young female patients of childbearing age do not have to use coumadin during pregnancy (coumadin is a teratonegic drug, it is not used for pregnant women) is one of the biggest advantages.
It is interesting that tissue valves are not accepted by the body as a foreign substance and therefore do not require the use of special anti-reaction drugs.
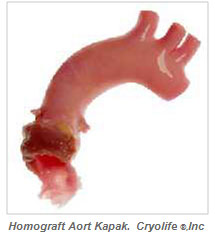
Tissue valves, including human ones (homograft / cadaver donated valves), operate silently, making no sound when opened and closed.
– Disadvantages Tissue heart valves are not lifelong valves. Interestingly, the lifespan of the valves is also related to the age of the patient. In fact, young patients are faster to deposit calcium deposits on the valves than the elderly. The lifespan of the bioprosthetic heart valves we use is between 15-20 years. For patients with a bioprosthetic valve, a second operation could be required and the risks that a second operation may bring are the most important disadvantages.
Pregnancy protocol for patients with heart valve surgery
A standard approach for patients with metal valve replacement has not been mentioned. Yet the more accepted approach is to give LMWH (low molecular weight heparin) between 6-12 weeks, continue with coumadin before and after, and return LMWH two weeks before delivery. However, the necessity of surgery due to valve thrombosis during pregnancy should not be ignored in patients using LMWH during pregnancy. All these pose serious risks for both the mother and the child. In the light of this information, we believe that the best approach to ensure a healthy delivery is to provide detailed information to the patients and their relatives about the treatment options, the risks for the child and mother, and to leave this important decision to the family. As a team, we recommend a direct bioprosthetic valve to our patients who are of childbearing age and who want children. We stop the coumadin at the 6th month of the operation. Many of our patients have had children without any problems this way. An average of 25-30 years of use is reported for new generation bioprosthetic valves.
Our recommendation:
We evaluate each patient separately, however we usually recommend tissue valves. This is due to the risks associated with long-term use of Coumadin.
Age is an important factor. We always recommend using a tissue valve for aortic valve replacement in patients over the age of 70 and with concomitant problems such as coronary artery disease.
We make decisions for young patients by taking their lifestyle and concerns into account.
We tell our patients about the risks of long-term anticoagulant use (in mechanical valves),
We explain the risks that a second operation could cause (in bioprosthetic tissue valves).
We have suggestions about the choice of valves, but after explaining the valve options to the patient, we give them time to discuss the issue and decide with their families.
It is worth remembering that mechanical (metal) valves can give excellent results in selected cases. Patients consciously continue coumadin treatment and if PT-INR values are kept at the desired level, they continue their lives without any problems.
For example, we whole heartedly recommend the mechanical prosthetic valve for young males whose mitral valve we cannot repair or female mitral valve patients who have completed their reproductive cycle.
There are also cases where a mechanical valve is the best solution, such as for young, male or female aortic valve patients who have completed their reproductive age.
